
Neuropsychologist Javier Tomas Romero presents some principles for developing instructions in cognitive rehabilitation. Direct instructions and programmed instructions, their design and which produce the greatest effect.
Below we will present some principles for creating instructions in your cognitive rehabilitation activities. If what you intend is to personalize the activities (which does not have to be the case), instructions are an important part you should work on for your patient. Adapting instructions to the characteristics of learning requires effort since you must understand the way your patient thinks, reasons, and learns. For this reason we describe several methods from the scientific literature.
Direct instruction and programmed instructions
The main methods of instruction are (Ehlhardt, Sohlberg and Glang and Albin; 2005):
Direct instruction
It is a structured instruction method that does not aim to monitor the patient’s thinking. Some of the main direct instruction methods are:
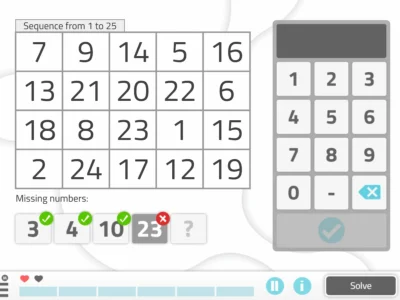
- Step-analysis (sequences)
- Modeling
- Massive feedback
- Massed practice: there are three types; massed, mixed and spaced
- Spaced action diagrams
- Observation of models
- Errorless learning
Programmed instructions
Their goal is for patients to learn to monitor their thinking. They are part of metacognitive skills. Obviously they cannot be applied to all patients as a minimum level of comprehension, language, reasoning, prospective memory, planning, etc., is required, so you must adapt the instruction to the patient’s cognitive level or profile. Some main methods are:
- “Scaffolded” method: involves creating flows or diagrams. They are graphical representations of the thought process.
- Metacognitive strategies
- Estimates (of abilities)
- Self-monitoring and control processes (by comparison in the task)
- Attributions (about task performance, possible complications in the task, resources…)
- Problem analysis
- Expectation training
- Self-instruction sequences
- Verbal self-regulation

Subscribe
to our
Newsletter
Design of cognitive rehabilitation instructions (Sohlberg, Ehlhardt, Kennedy, 2005).
Instructions must meet a series of criteria:
- Content analysis to detail the “big ideas”, concepts, rules, and generalizable strategies.
- Determine necessary skills and prerequisites.
- Sequence competencies from simple to more complex.
- Develop task analyses.
- Develop and sequence a wide range of training examples to facilitate generalization.
- Create simple and consistent instructions using clear language and script them to reduce confusion and to focus the learner on the relevant content.
- Clearly establish the learning objectives
- Establish achievement criteria
- Provide models and gradually establish fading of cues and prompts to facilitate errorless learning.
- Pre-correction by instructing the pre-required capacities for the task first, or by isolating the difficult steps of the instruction.
- Provide consistent and rapid feedback (give the “good” model immediately if the patient makes an error).
- Provide large amounts of correct massed practice followed by distributed practice.
- Provide sufficient and cumulative review (integration of new and old material).
- Individualize the instruction (language, pace, time, abilities…)
- Progressive assessment of behavior to evaluate functional evolution.
A combined model (direct instruction and programmed instruction) produces the best results (Ehlhardt, Sohlberg, Glang, Albin; 2005). After this type of model, and in order of demonstrated effectiveness, we find:
- The strategy in programmed instructions.
- Direct instruction.
- Non-direct instructions (e.g., social skills training or trial-and-error).
Which instructions produce the greatest effect?
- Explicit practice: distributed practice and review, repeated practice, review of sequenced performance, continuous feedback and reviews.
- Task orientation/advance organizers: setting instructional goals, reviewing materials prior to instruction, instructing attention to particular information, providing advance information about the task.
- Presentation of new material for learning: diagrams, mental representations, information about previous performances that relate to the task you are going to carry out with the patient.
- Modeling steps to complete the task.
- Sequencing
- Systematic investigation/validation and reinforcement: use of validations and continuous feedback. You should make your patient ask themselves the consequences of performing behaviors in certain situations and tasks. When you present a consequence, it is better to start with negative reinforcement (which has a more generalized effect) and end with positive reinforcement (which produces greater benefits in recovery).
These are some of the methods and principles you can adapt for your patient. The following post focuses on the scaffolded method (literally, it means scaffolding) for rehabilitation.
If you liked this post about instructions in cognitive rehabilitation, you might be interested in these NeuronUP articles.




“This article has been translated. Link to the original article in Spanish:”
Instrucciones en rehabilitación cognitiva: métodos, diseño y eficacia
 The Confabulation Phenomenon (Volume II): Theoretical Models
The Confabulation Phenomenon (Volume II): Theoretical Models


Leave a Reply